
SPECIALTY GROUPS
DIASTASIS RECTI
DRA is the most common problem seen after pregnancy (especially after multiple pregnancies) and the biggest thing to try and prevent during pregnancy
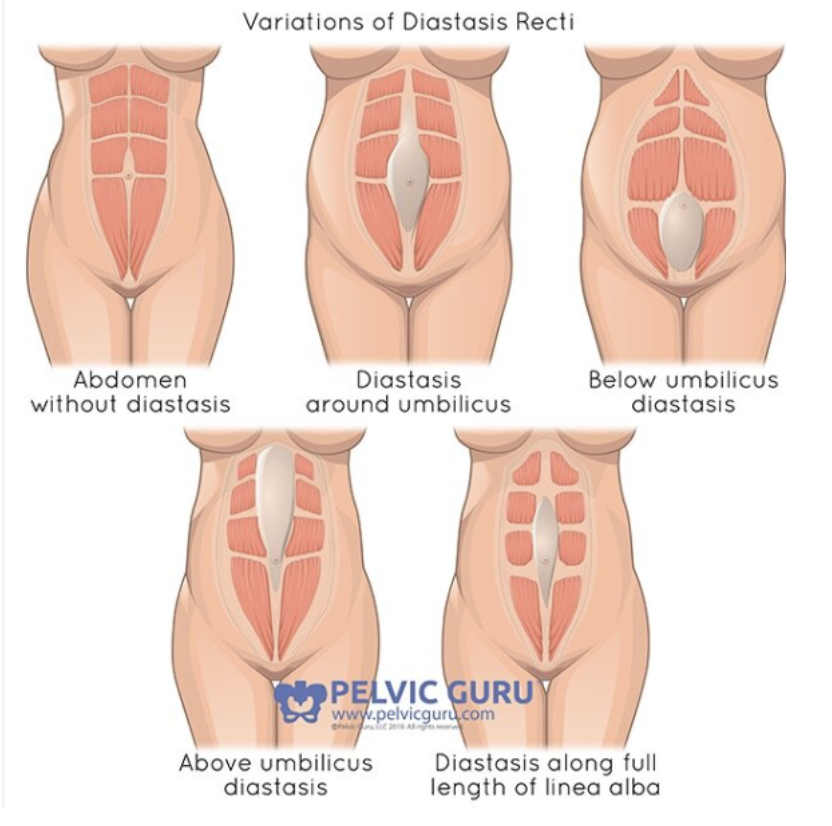
DRA is the stretching or separation of the rectus abdominis or “six-pack muscles"” caused by the thinning of the midline connective tissue (linea alba). This thinning leaves abdominals unsupported and causes air to push against the sides of the rectus abdominis.
Think of the linea alba (what connects both sides of the core) as a piece of laffy taffy. Every time it stretches, it does not always come back to its original strength and position.
Most separations heal on their own after birth, but some remain.
ALL CRUNCHES and excessive repetitive twisting movements should be avoided while clients have more than 1 inch of DR.
If extreme DR encourage the SIDE ROLL position when getting up after lying down
HOW TO CHECK FOR DRA
Client will lie flat on their backs with knees bent
Client will place fingers on their navel, pointing towards pelvis, and press down
Client will lift head up about an inch while keeping shoulders on the carriage
If client has DRA, they will feel a gap between the muscles that is ~2 fingers or greater
Any separation per client must be added to profile as an additional note
DR MOVES THAT SHOULD BE SAFE
-
**Moves at the back are dependent on whether or not they’ve mastered at the front. Ideally we want to keep clients at the front until they have about 1 inch or less of separation
Planks (knees)
Wheelbarrow
Carriage Wheelbarrow
BC & BP Wheelbarrow once truly mastered at the front
Cobra
Carriage Wheelbarrow
Saw
Carriage Saw
BC & BP Saw once truly mastered at the front
Scoop
Mini Scoop
High Bar Plank Crunch
Back High Bar Plank Crunch once mastered at the front
High Bar Plank to Pike
Back High Bar Plank to Pike when mastered at the front
Carriage Super Crunch (elbows on carriage)
Heavy Plank Crunch (knees)
Resistance Plank (knees)
-
Recommendation is to hold in plank cardio moves to reinforce control and stability.
-
Here are your go to DR friendly oblique moves. If there is a (*) next to the name, that move has a slight video variation:
Side Plank (no crunch/twist variations)
Carriage Side Plank (no crunch/twist variations)
Twisted Wheelbarrow
Carriage Twisted Wheelbarrow
Twisted Cobra
Carriage Twisted Cobra
Twisted Saw
Carriage Twisted Saw
Side Plank
Carriage Side Plank
Bird Dog (done at the front either platform or carriage facing)
High Bar Twisted Plank Crunch
High Bar Butterfly Plank Crunch
High Bar Chopsticks
Oblique Sweep
Froggy Kicks
Mermaid
Carriage Mermaid
Bicycle Twist ((*) no twist)
Carriage Bicycle Twist ((*) no twist)
Kneeling Torso Twist (*)
Tailbone Chest Fly Twist (no twist - chest focus - criss cross legs)
Lunging Torso Twist (no twist same mod as Kneeling Torso Twist)
-
ALL LUNGES SHOULD BE DR SAFE
-
ALL LEGS SHOULD BE DR SAFE
-
ALL ARM EXCEPT TAILBONE MOVES & CRUNCH MOVES SHOULD BE DR SAFE:
SIT CROSS LEGGED:
Tailbone Chest Fly
Rear Delt Chest Fly
Tailbone Bicep Curl
REMOVE CRUNCHES FROM:
Heavy Bicep Curl
Carriage Row
WHAT IS CONING?
Coning (or doming) happens when pressure pushes outward through the midline of the abs instead of being supported by the deep core (TA + pelvic floor). You’ll see the belly rise or “tent” down the center during effort.
HOW TO SPOT (WHAT TO WATCH FOR)
A ridge or dome along the linea alba
Belly popping forward during slow, high-tension moves
Client holding breath or gripping through glutes/hip flexors
Happens most in: planks, crunches, pikes, heavy leg work, slow tempo
WHY IT MATTERS
Coning = poor pressure management
Over time it can:
Reinforce weak deep core engagement
Increase low back or pelvic floor issues
Reduce effectiveness of the movement
WHAT TO DO IF A CLIENT EXPERIENCES CONING
1. Cue breath first
2. Reduce the load
Shorten range of motion
Slow the tempo less
Knees down / lighter springs
3. Regress the movement
Swap crunch → heel press or tabletop movements
Swap plank → incline plank or kneeling variation
4. Rebuild correctly
Focus on exhale + tension before movement
If coning continues → the move is too advanced right now
IF DRA IS NOT IMPROVING
If DRA is not improving or clients are still experiencing back pain after at least 6-8 weeks it is best to check with an OBGYN or surgeon as a hernia or other complications may be present. Again we are not medical professionals so never diagnose.